

The Biophysicist Who Accidentally Found a Cancer Drug
How a failed experiment with platinum electrodes and bacteria led to one of oncology’s most important drugs

Barnett Rosenberg wasn’t looking for a drug. In his Michigan State University lab in 1965, he was chasing a speculative idea about electromagnetism and cell division. The mitotic spindle resembled the field lines between two poles, he reasoned. Maybe electric fields helped pull chromosomes apart during replication.
Simple experiment. Platinum electrodes in a chamber of E. coli growing in ammonium chloride solution. Current on.
Division stopped. The cells didn’t die, though. They kept growing, stretching into grotesque filaments up to 300 times their normal length.1 Under the microscope, what should have been neat bacterial rods looked like tangled spaghetti.

The Wrong Answer, Then the Right One
Rosenberg’s first interpretation was the obvious one: the electric field blocked division. He spent two years testing that hypothesis before the evidence forced him somewhere else entirely.2
It wasn’t electricity. Platinum was leaching from the electrodes into the growth medium, forming soluble coordination compounds in the ammonium chloride solution. Two more years went to identifying which platinum species was responsible.
The culprit turned out to be a molecule that inorganic chemists already knew: cis-diamminedichloroplatinum(II). Two ammonia groups and two chloride ions arranged around a central platinum atom in a flat, square geometry.1 Alfred Werner had characterized platinum complexes decades earlier. No one had thought to test them against living cells.
What made the finding stranger still: the trans isomer, identical in composition but with its chlorides on opposite sides of the platinum center, did almost nothing to bacteria. Geometry at the atomic scale separated inert from lethal.
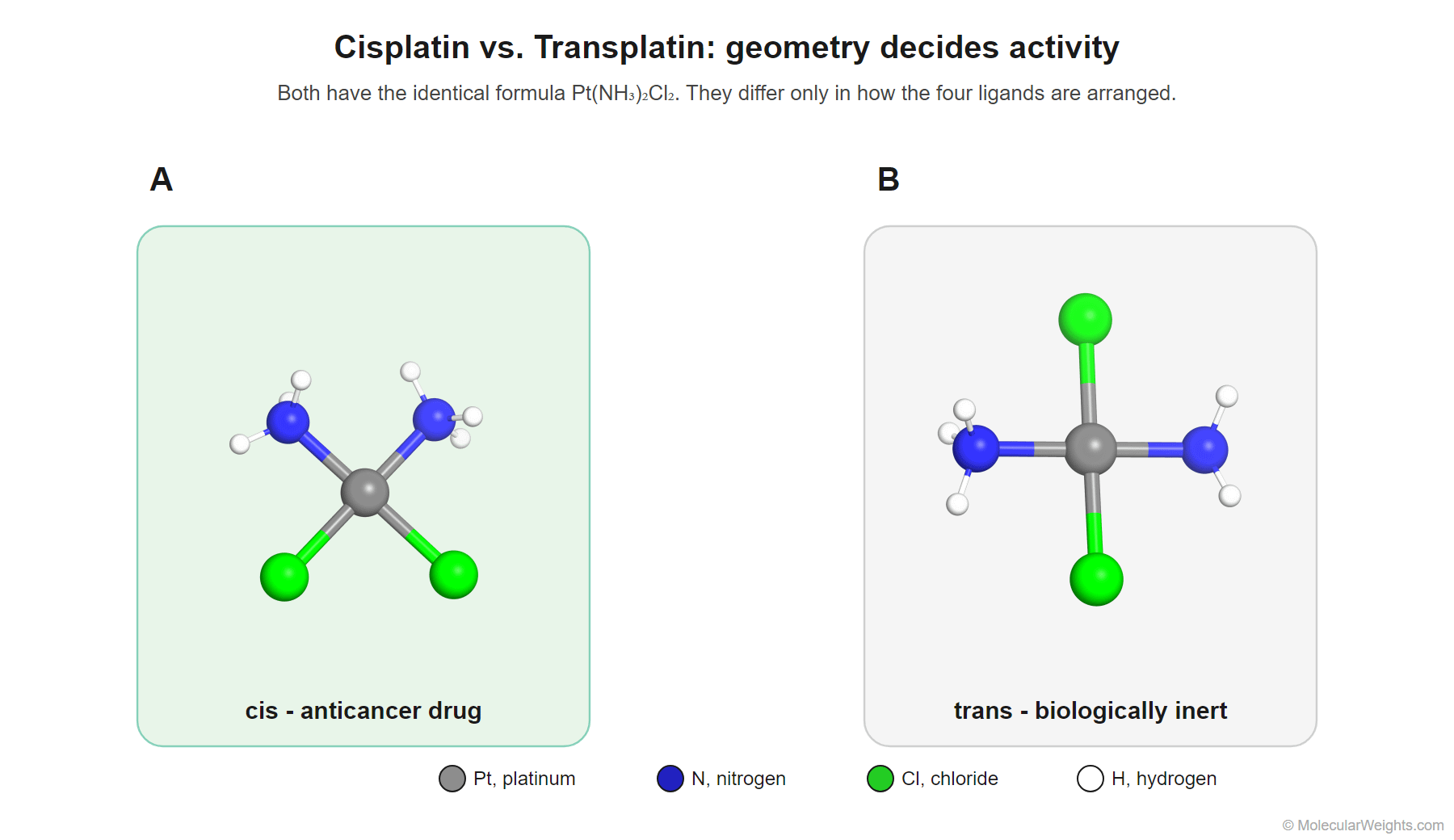
Figure 1. Cisplatin and transplatin share the formula Pt(NH₃)₂Cl₂ but differ in geometry: in the cis form the two chlorides sit adjacent (90° apart), in the trans form they sit opposite (180° apart). Only the cis isomer is an active anticancer drug.
A Trojan Horse Gated by Salt
The mechanism, worked out over the following decades, is subtler than four atoms around a platinum center might suggest.3
Cisplatin enters the bloodstream inert. Chloride concentration in blood plasma sits around 100 millimolar, high enough to keep both chloride ligands firmly bound to the platinum center. The molecule circulates without reacting.
Inside a cell, conditions shift. Intracellular chloride drops to roughly 4 millimolar.3 At that concentration, water molecules displace the chlorides one at a time, generating a positively charged, highly reactive platinum species. The drug activates only after crossing the membrane. A chemical Trojan horse, gated by a concentration gradient that the cell maintains for its own purposes.
The activated complex is an electrophile hungry for electron-rich targets. It finds them on D
NA, at the N7 nitrogen of guanine bases. One chloride displaced, one guanine bound. The second chloride leaves, and platinum grabs a neighboring guanine on the same strand.3,4
Two adjacent guanines, locked together through a platinum bridge. The helix bends by about 35 degrees at the kink. Replication machinery stalls. Repair enzymes try to fix the distortion but often fail, and when enough crosslinks accumulate, the cell triggers apoptosis, programmed self-destruction.3
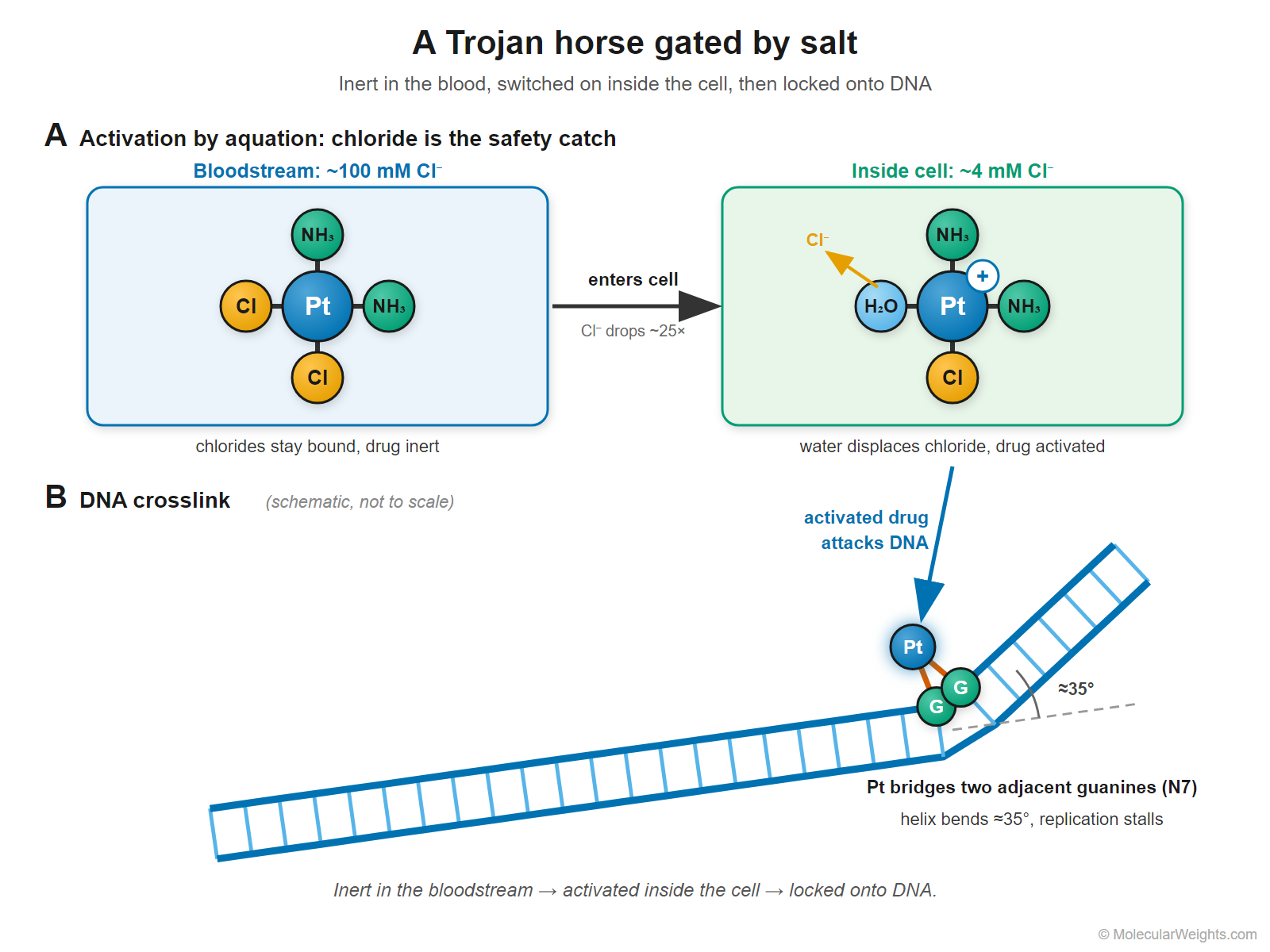
Figure 2. Cisplatin circulates inert in the chloride-rich bloodstream. Once inside a cell, where chloride is far lower, water displaces a chloride to form a reactive, positively charged complex that bridges two adjacent guanines on the same DNA strand, kinking the helix and stalling replication.
Rapidly dividing cells encounter these crosslinks most often because they copy their DNA most frequently. Cancer cells replicate faster than most healthy tissue. That differential, imperfect as it is, gives cisplatin its therapeutic window.
From Filaments to a 95% Cure
Rosenberg published the bacterial findings in Nature in February 1965.1 Four years later, he and colleagues reported that cisplatin shrank sarcoma 180 and leukemia L1210 tumors in mice, with no recurrence at six months.5 The National Cancer Institute funded Phase I trials beginning in 1971.
The transformation came from Lawrence Einhorn at Indiana University. Starting in 1974, Einhorn treated men with disseminated testicular cancer using cisplatin combined with vinblastine and bleomycin. Before those trials, the cure rate for metastatic disease hovered around 5%.2,6
Einhorn’s Phase II results: 85% of patients disease-free.6 He later called it “a one logarithmic increase in the cure rate.”2 The FDA approved cisplatin in 1978. Testicular cancer death rates have since fallen by two-thirds, and the overall cure rate now exceeds 95%, making it the most curable solid tumor in oncology.2
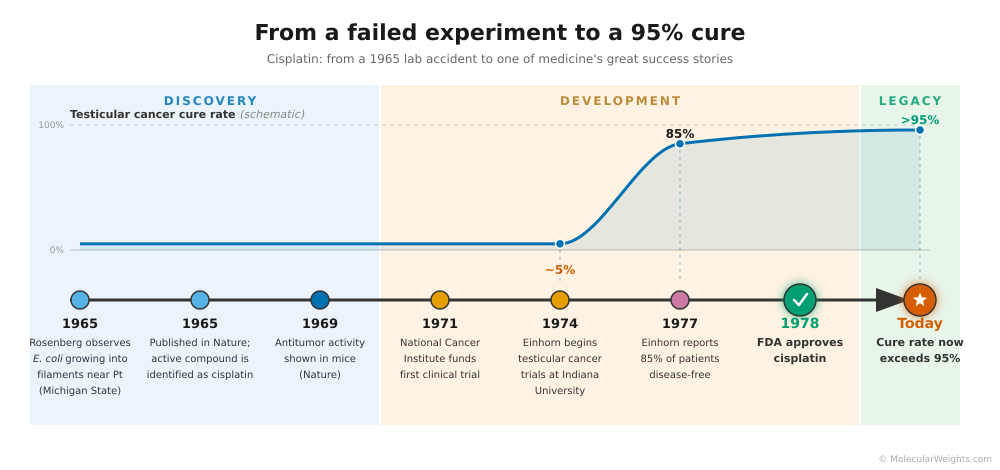
Figure 3. From Rosenberg’s 1965 observation of filamentous bacteria to FDA approval in 1978 and today’s cure rate above 95%, cisplatin moved from lab accident to the most curable solid tumor in oncology.
Beyond testicular cancer, cisplatin became first-line therapy for ovarian, bladder, lung, and head and neck cancers. Roughly half of all chemotherapy regimens today include a platinum-based drug.4
The Costs, and What Came After
Cisplatin is not gentle. Kidney damage limits how much can be given. More than a third of adult patients develop hearing loss; in children the rate climbs above 60%.3 The nausea was severe enough in early trials to become notorious among oncology nurses.2
Resistance emerges in many tumor types. Cells pump the drug out or repair crosslinks before they can trigger cell death.4 Carboplatin arrived as a less toxic alternative for situations where the side-effect trade-off matters. Oxaliplatin extended the platinum family’s reach to colorectal cancer. But for testicular cancer, where cure is the goal and potency is paramount, cisplatin remains the standard.4
By the numbers
· Cisplatin molecular weight: 300.01 g/mol
· Testicular cancer cure rate before cisplatin (1974): ~5%
· Testicular cancer cure rate today: >95%
· Time from Rosenberg’s observation to FDA approval: 13 years
· Platinum-based drugs now treat more than a dozen cancer types
Sixty years after Rosenberg watched his bacteria refuse to divide, cisplatin remains among the most prescribed chemotherapy agents on Earth. The molecule is small: four ligands arranged around a platinum center in a geometry that Werner would have recognized in 1893. That something so structurally spare can distinguish the inside of a cell from outside, can find two adjacent guanines in a genome of billions of base pairs and lock them together, still impresses.
Rosenberg wasn’t trying to cure cancer. He was trying to understand cell division with a pair of platinum electrodes that were supposed to be inert. They weren’t. And that failure became one of medicine’s great accidents, right alongside a contaminated Petri dish in 1928.
References
Rosenberg B, VanCamp L, Krigas T. (1965). Inhibition of Cell Division in Escherichia coli by Electrolysis Products from a Platinum Electrode. Nature 205(4972):698–699. PMID 14287410
National Cancer Institute. The “Accidental” Cure: Platinum-based Treatment for Cancer: The Discovery of Cisplatin. cancer.gov
Dasari S, Tchounwou PB. (2014). Cisplatin in cancer therapy: molecular mechanisms of action. Eur J Pharmacol 740:364–378. PMC4146684, free full text
Kelland L. (2007). The resurgence of platinum-based cancer chemotherapy. Nat Rev Cancer 7(8):573–584. PMID 17625587
Rosenberg B, VanCamp L, Trosko JE, Mansour VH. (1969). Platinum Compounds: a New Class of Potent Antitumour Agents. Nature 222(5191):385–386. PMID 5782119
Einhorn LH, Donohue J. (1977). Cis-diamminedichloroplatinum, vinblastine, and bleomycin combination chemotherapy in disseminated testicular cancer. Ann Intern Med 87(3):293–298. PMID 71004
For Further Reading
Accessible: National Cancer Institute overview of cisplatin development. cancer.gov
Deep Dives: Dasari S, Tchounwou PB. (2014). Cisplatin in cancer therapy: molecular mechanisms of action. Eur J Pharmacol 740:364–378. Free full text: PMC4146684 - Kelland L. (2007). The resurgence of platinum-based cancer chemotherapy. Nat Rev Cancer 7(8):573–584. PMID 17625587
Topline image modified from structure in the Protein Databank PDB ID: 1AIO